No products in the cart.

Image used with permission of Cardiac Science
AED Request
You may save a life by making sure you have an AED
If defibrillated within the first minute of collapse, the victim’s chances for survival are close to 90 percent. For every minute that defibrillation is delayed, survival decreases by 7 percent to 10 percent. If it is delayed by more than 10 minutes, the chance of survival in adults is less than 5 percent.
How to Use an AED
Here are some videos from Cardiac Science on how to use their G3 and G5 AED units.
AED Request Form
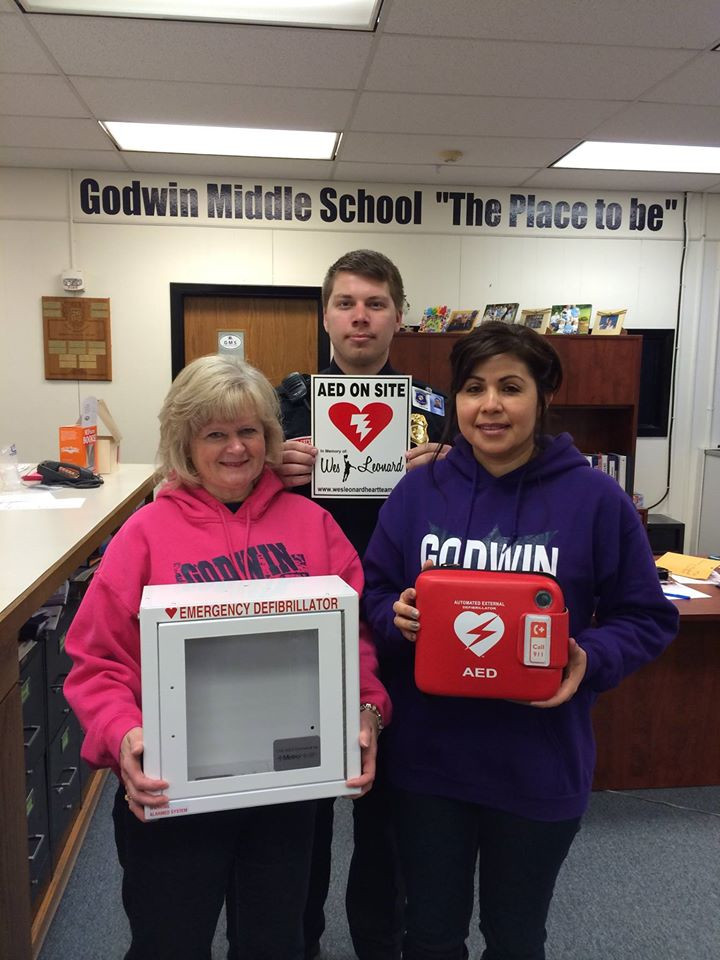
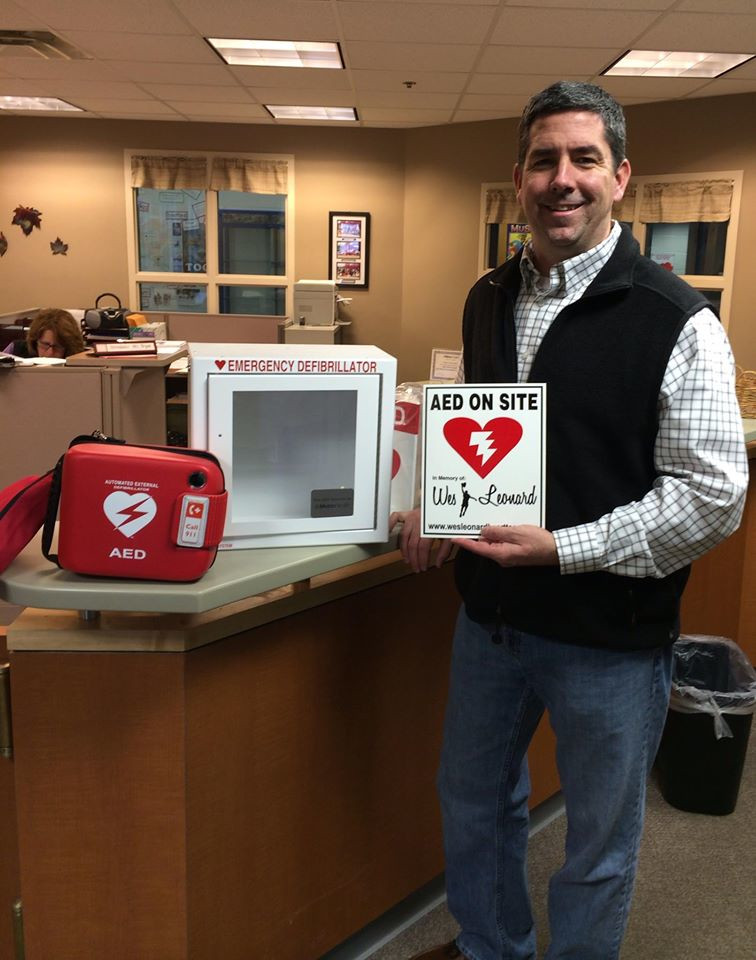
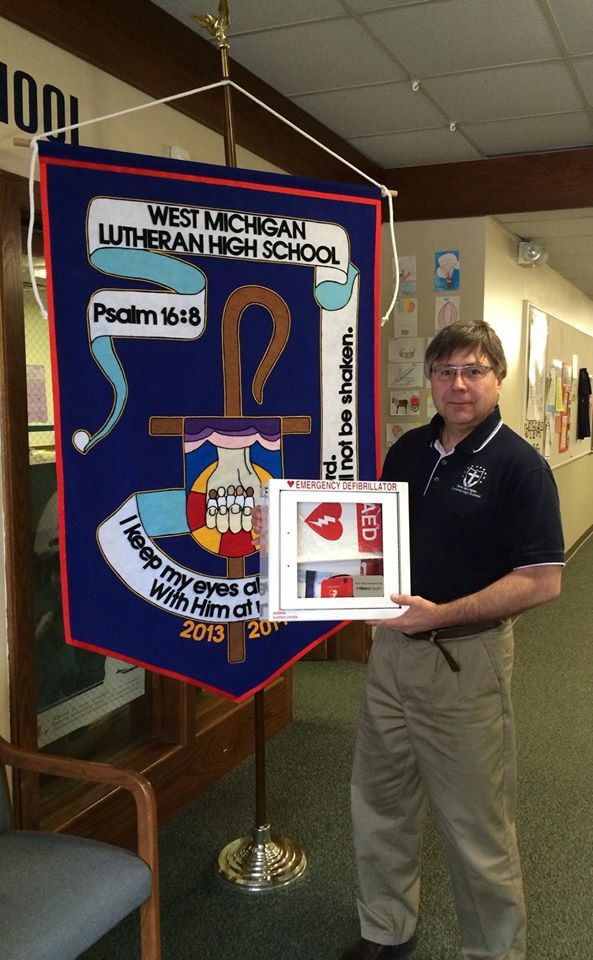
Donated AEDs
AEDs donated by the Wes Leonard Heart Team